- Home
- China
- World
- Europe
- Politics
- Business
- Opinions
- Tech & Sci
- Culture
- Sports
- Travel
- Nature
- Picture
- Video
- Live
- TV
- Specials

Share

Copied

The COVID-19 pandemic has touched every corner of the world. More than 1.27 million people have tested positive as of April 6. The death toll has passed 69,300. Many more are expected to be affected before the crisis is over.
The global public health emergency raises a multitude of questions about the preparedness of countries across the planet.
Italy, the United Kingdom and United States were ranked in the top 30 by The Lancet's 2018 Healthcare Access and Quality Index (HAQ), with China at 48.
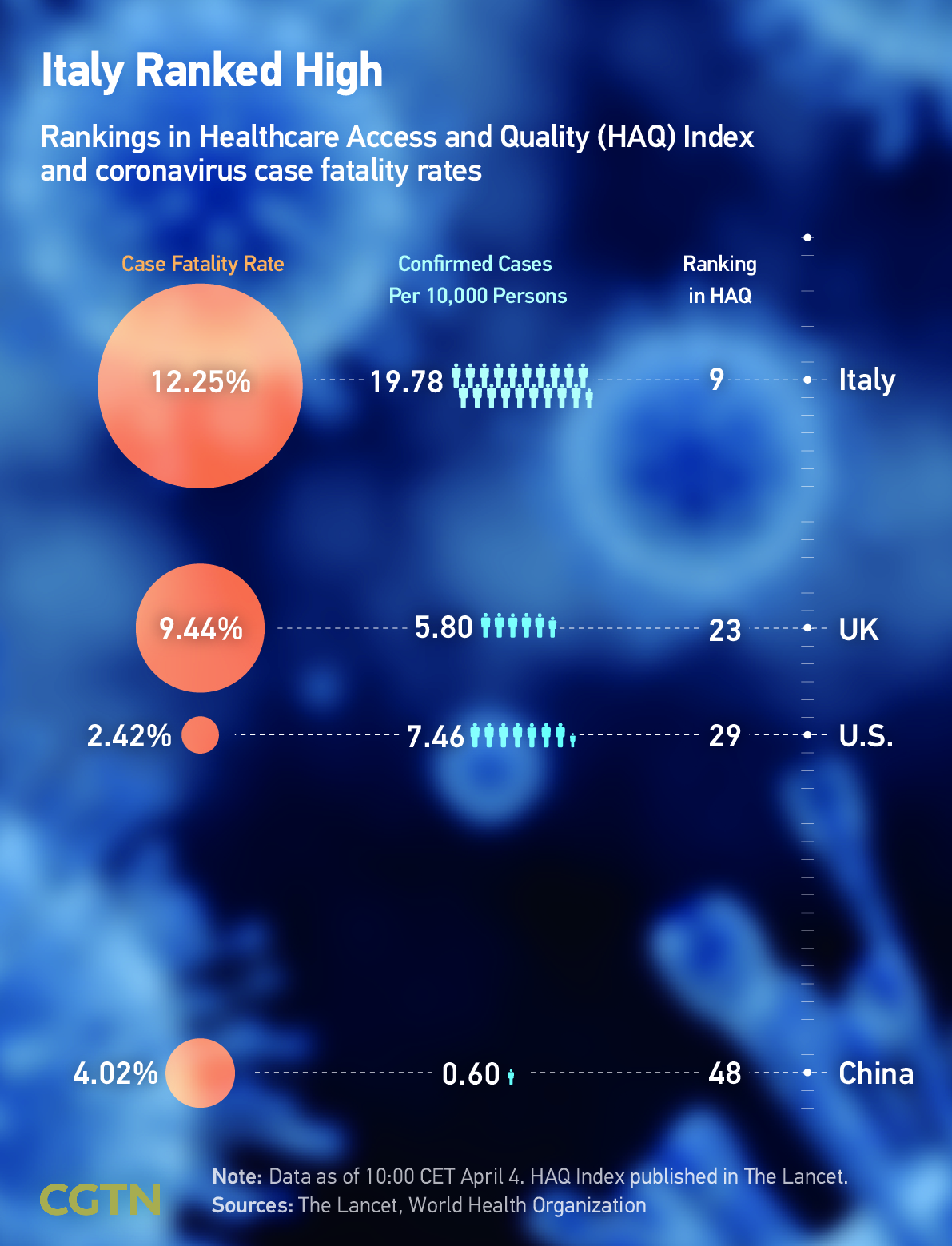
But rankings such as the HAQ appear as poor indicators of a country's preparedness for a pandemic. Were health systems around the world ready for such a grave challenge?
Challenge One: Decreasing long term funding
Mitigating the human cost of the pandemic requires huge resources. Trillions of dollars are being plowed into countries to deal with COVID-19 and its fallout. But could more of that sum have been spent in preparation?
In Italy, which has been hit particularly hard, the ratio of health expenditure to gross domestic product (GDP) has been decreasing for three consecutive years, according to the World Health Organization (WHO).
The funding cuts meant that even before the virus hit, the country faced a shortage of thousands of doctors and nurses, Costantino Troise, the head of the medical union Anaao Assomed told the Washington Post.
And in the UK, which is now losing hundreds of lives per day, data from NHS England shows that the National Health Service has been under pressure, with 15.2 percent of patients waiting for treatment for longer than 18 weeks last year. That number was only eight percent when the waiting time target was introduced in 2012.
Challenge Two: Absence of leadership and expertise
The U.S. ranked first in the ratio of health expenditure to GDP in the world in 2017, according to data from the WHO. Levels of investment in healthcare were high, even if questions about the efficiency of the system persist.
But the country is now the epicenter of the pandemic and its hospitals are under severe strain. On top of systemic healthcare failures, there have been mixed messages from the top and a series of questionable decisions on government bodies and personnel in recent years.
In 2018, President Donald Trump dissolved the office of National Security Council Directorate for Global Health Security and Biodefense.
It was established to prepare for the next disease outbreak and prevent it from becoming an epidemic or pandemic, the former senior director of the office Beth Cameron wrote in an article published in the Washington Post on March 13.
Challenge Three: Medical capacity overloads
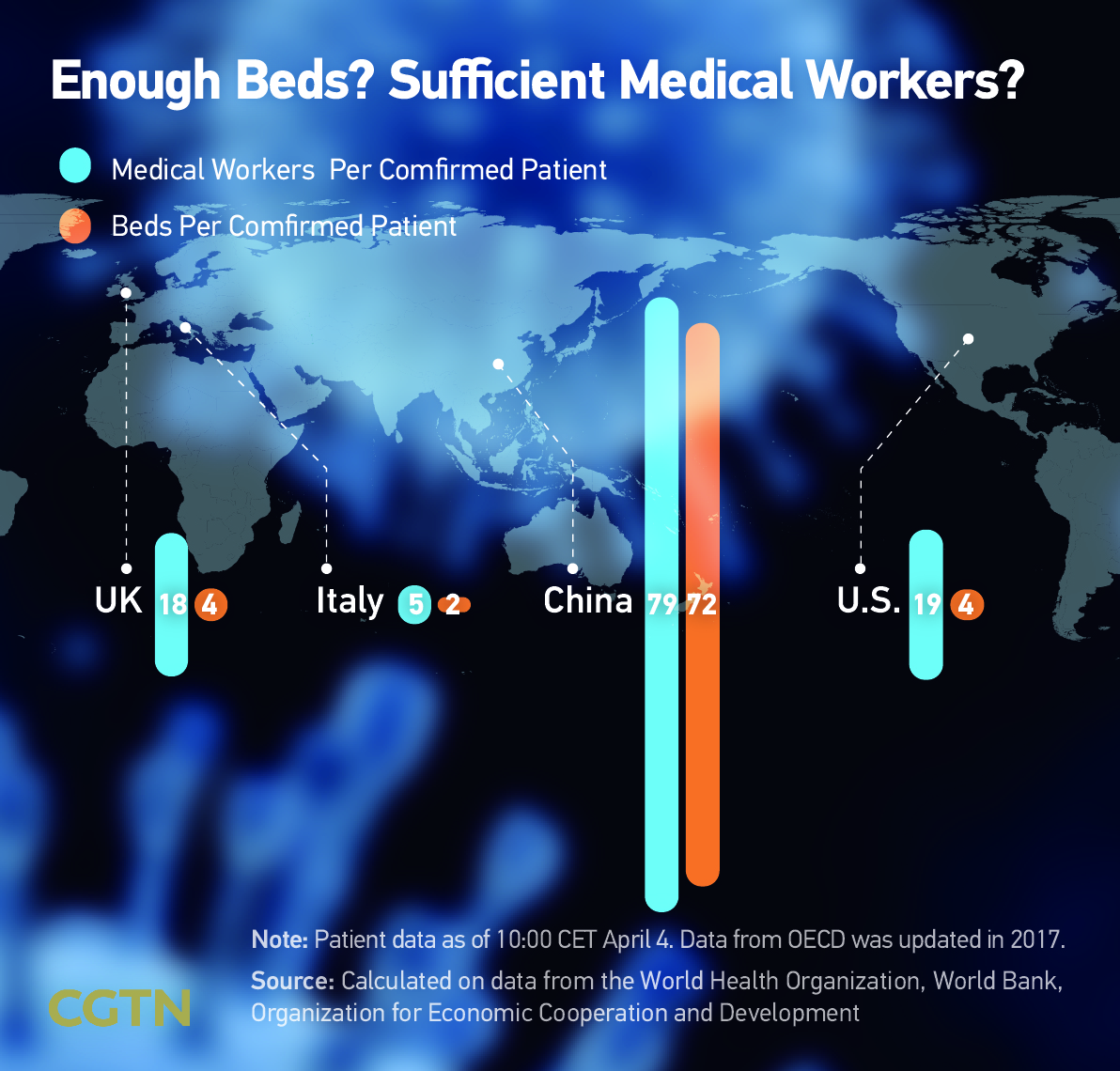
The rapid spread of COVID-19 has stretched existing medical capacity to breaking point in many countries.
A comparison of the ratio of confirmed patients to hospital beds and medical staff in China, Italy, the U.S. and the UK, suggests China has the lightest burden. A confirmed COVID-19 patient can be nationally allocated to 79 medical staff and 72 beds in theory, if non-COVID-19 sufferers are discounted.
However, COVID-19 overloaded the health system in Wuhan, China's hard-hit city. There weren't enough beds or medical workers at the early stage of the outbreak. On February 4, Wuhan was left with 305 available beds but 1,967 confirmed patients waiting for treatment.
The epidemic coincided with China's Spring Festival, when production in many factories was suspended. The resumption of work and national logistics was delayed, resulting in a slowdown in the production and distribution of medical supplies.
As factories reopened, temporary hospitals were built and medical workers were sent to the hard-hit area, the pressure on the system was relieved.
Challenge Four: Equipment: Personnel imbalance
An abundance of medical equipment is vital in a pandemic, but if there aren't enough doctors and nurses the efficacy of the supplies is reduced.
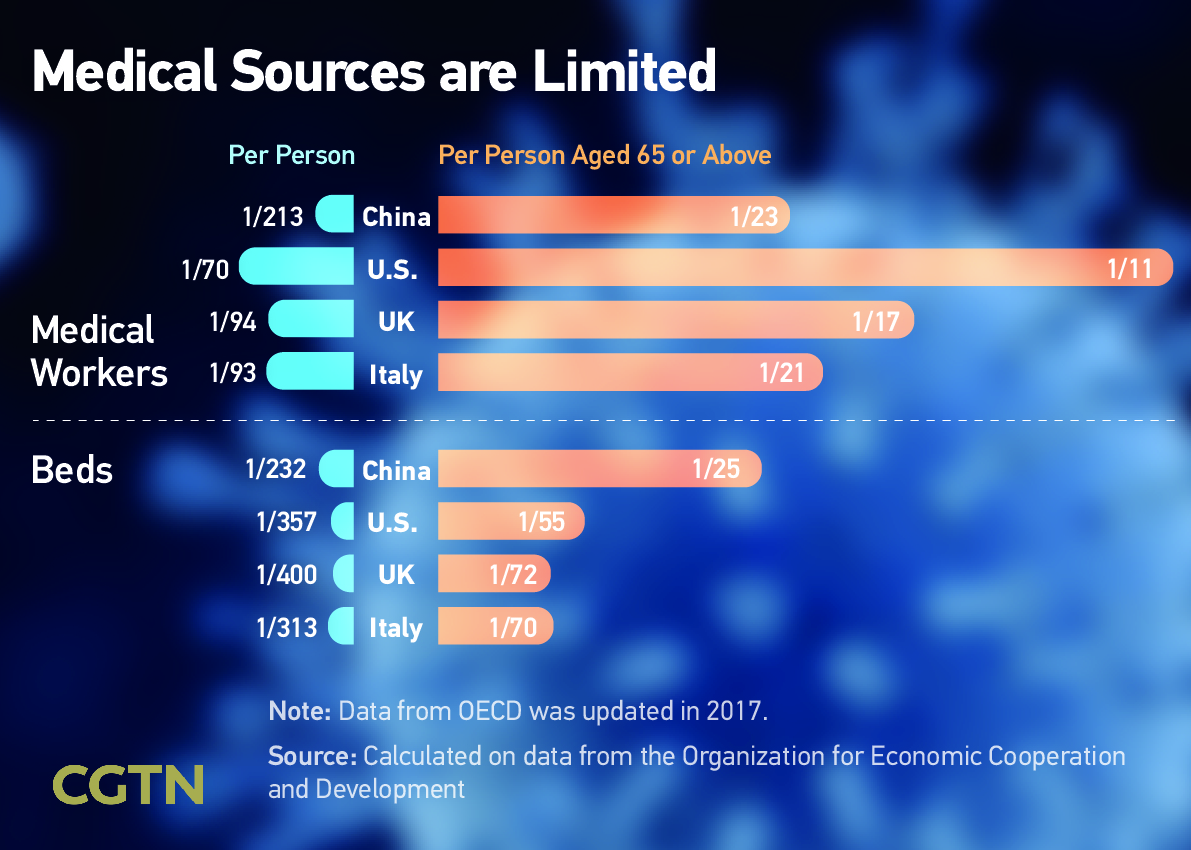
Per capita, China's hospital beds to total population ratio is slightly lower than in the U.S., the UK and Italy. But by comparison with those countries, China lacks medics.
The number of medical personnel per capita is only 1:213 in China, far lower than that of the other countries. The shortage of medical staff makes it difficult for China to give full play to its strengths in medical equipment, pharmaceutical manufacturing and other aspects in the fight against the pandemic.
Challenge Five: Demographic disparities
People aged 65 or above are particularly vulnerable to COVID-19.
The ratio of beds per elderly person in China is much greater than in the other three countries, due to differing demographics. A person in the 65+ group competes with 69 others for one hospital bed in Italy and the number in China is 24, discounting the needs of younger people. Some older COVID-19 patients in Italy reportedly gave up medical treatment to younger sufferers, who are more likely to survive.
Governments can do everything possible to control the disease during the emergency period, but deep-rooted problems in health infrastructure need to be fixed for countries to be better prepared. To truly improve the capacity of health systems and equip the world for pandemics, there are lessons to be learned and there is work to be done.
Text by: Bai Yu, Han Mo
Data Collection: Li Jingyi
Designer: Yu Pianyi
Data Checker: Zuo Lin
Senior Producer: Bi Jianlu
Supervisor: Mei Yan
(If you want to contribute and have specific expertise, please contact us at opinions@cgtn.com.)